


Listen to this article:
0:000:00
Your browser does not support the audio element.
Despite an aging population with an increasing number of chronic conditions, the use of the Medicare home health benefit has declined in recent years due to various factors including payment incentives favoring less medically complex patients, Medicare Advantage referral rejections and staffing shortages. This raises concerns about beneficiary access to care, according to a new issue brief from the Commonwealth Fund.
“Declining utilization in the traditional Medicare home health benefit not only reflects lower enrollment but also the effects of payment policy and quality incentives,” the issue briefsaid. “These factors — together with Medicare Advantage underpayment, narrow networks and utilization controls, agency referral practices and availability, and workforce shortages — may limit access for beneficiaries who could benefit most from home-based care and thereby increase utilization of higher-cost institutional settings or caregivers.”
For the brief, researchers for the Commonwealth Fund, a nonprofit foundation that supports independent research on healthcare policy issues, interviewed more than 20 policy experts in traditional Medicare, MA and aging and disability policy, as well as home health agencies, providers and advocates, between November 2025 and February 2026. They also conducted a review of published reports on payment and quality, access and utilization.
Home health coverage, a Medicare benefit since the program’s inception in 1965, with services designed to help beneficiaries stay in their homes while avoiding more costly institutional care, continues to decrease
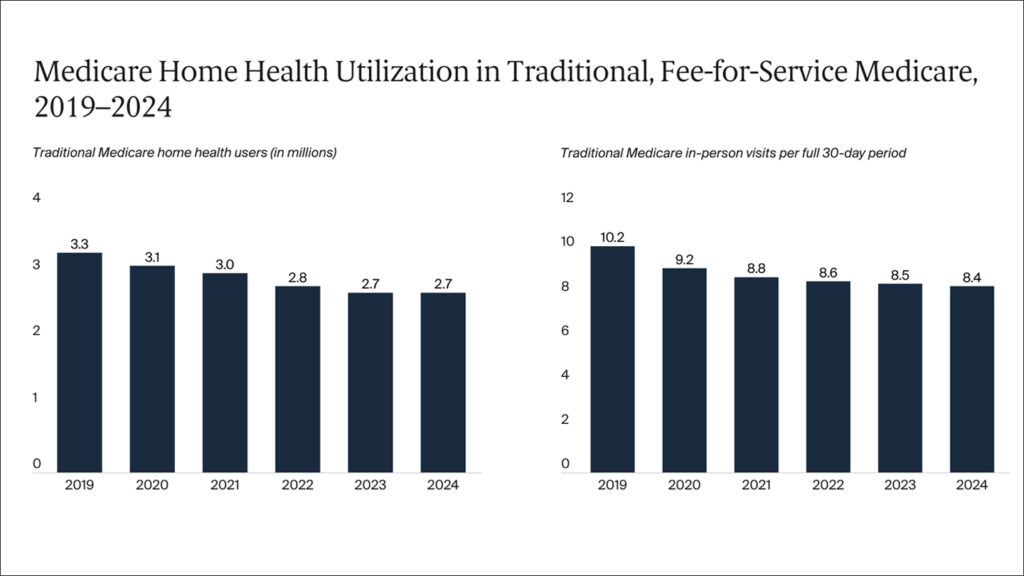
“Despite a growing, aging population, use of the Medicare home health benefit has declined in recent years, particularly for home health aide and medical social services,” the researchers noted. “Declining use disproportionately impacts community-admitted patients, who experience longer stays, are more likely to be older, rural, and dually eligible for Medicare and Medicaid, and are more likely to be living with Alzheimer’s disease and related dementias compared to post-institutional patients. It’s noteworthy that between 2020 and 2022, home healthcare use decreased among individuals with dementia.”
Payment disincentives
Based on their research, they found Medicare utilization for home health services is declining due to multiple, interrelated factors. One of the reasons is that the current payment system tends to favor short-term beneficiaries over those with longer-term chronic conditions. Under the Patient-Driven Groupings Model (PDGM), which was instituted in 2020, home health agencies are paid for 30-day periods of care, with 60-day recertification. The researchers said the payment model tends to favor shorter term periods of care and post-acute referrals, which tend to involve patients who are expected to show rapid improvement and not those with chronic conditions.
“My biggest overarching concern about PDGM is it has really focused the benefit to be a short-term post-acute benefit for patients with simpler, less complex needs,” one of the researchers noted.
The researchers also found that home health utilization was lower among MA enrollees than traditional Medicare beneficiaries. They noted that MA utilization management tools, such as prior authorization, visit caps and frequent reauthorization requirements, created additional barriers for home health patients and MA plans were more likely to deny referrals of home health services than traditional Medicare
“I can tell you that we’ve seen referral rejection rates that are three, four times higher for certain MA plans than for traditional Medicare,” a home health agency representative told the researchers.
Staffing shortages were also identified as a major constraint to accessing care, with home health agencies facing difficulty recruiting and retaining staff, especially registered nurses, due to competition from hospitals offering higher wages and better benefits.
“Workforce shortages limit agencies’ capacity, particularly for beneficiaries with complex or chronic care needs, or those living in rural or underserved areas,” the research noted. “It is noteworthy that over 25% of referred patients were turned away by home health care providers due to staffing shortages.”
In their findings, researchers identified several policy considerations to improve utilization of home health services, which included:
- Better aligning traditional Medicare payment policy and quality measures with patient complexity and maintenance needs;
- Considering improvements to Medicare quality measures to ensure they fully reflect the needs of all beneficiaries, including those with chronic conditions and longer-term needs;
- Strengthening oversight and tracking systems to monitor for quality, timely initiation and referral completion;
- Improving transparency in MA home health access and payments, performance on functional outcomes, network adequacy and utilization management;
- Developing options for expanding the home health care workforce that include better payment and benefits, and immigration policies that enable qualified foreign workers, such as nurses and home health aides, to seek a legal pathway to working in US home health agencies;
- Considering options to mitigate caregiver burden and stress, such as respite care, training and payment.
The researchers also recommended that a survey be conducted of both traditional Medicare and MA beneficiaries who are referred for home health care services to better understand turned-down referrals and the reasons for declining utilization by demographic characteristics, health and functional status
“Misaligned payment and quality incentives, MA practices and workforce constraints can limit access to home health services for Medicare beneficiaries,” the researchers concluded. “Interviewed experts identified several policy options to increase access and reverse declining utilization, including better aligning payment with patient needs, improving oversight and transparency, and strengthening workforce capacity