


Szu Ping Chan
Sun, July 12, 2026 at 5:00 AM UTC

A teenager in crisis. An octogenarian managing multiple health conditions. A man with sudden chest pains
It’s just after 9am on Tuesday, and Greg, a GP, has already made decisions that could mean the difference between life and death
In less time than it takes to hang out the washing, he must assess, diagnose, prescribe or refer, write his notes and move on
Greg – not his real name – works three days a week and is one of the growing number of part-time GPs across England
In the Bristol, North Somerset and South Gloucestershire NHS healthcare region he works for, just 9.4pc of GPs work full-time – the lowest share in England. But it is far from an isolated problem
Telegraph analysis of NHS data shows that fewer than one in five GPs (19pc) now works full-time, down from 27pc in 2019
Even in Essex, where full-time work is most common, the figure is just 33pc
On paper, the answer looks simple. If every GP working three days a week or less added just one extra day, England would gain the equivalent of around 2,000 full-time doctors. That’s a 9pc boost to the workforce
But those figures tell only half the story. Interviews with medical staff reveal a profession stretched in every direction
GPs describe being buried under paperwork and fit notes while caring for patients with increasingly complex needs
They also warn that working more hours threatens to leave them out of pocket because of a tax system that punishes those who earn over £100,000
Burnout is driving experienced doctors out of the NHS, while senior colleagues warn newly qualified GPs against full-time work
Yet in one of the NHS’s greatest contradictions,qualified GPs are struggling to find permanent jobs
Something in the system is clearly broken
Picking up the pieces
Greg says the pressure isn’t just the number of patients, it’s how much work hospitals now expect GPs to pick up
One of his first patients on Tuesday is an 88-year-old woman who has recently been discharged from hospital after a fall that left her with multiple fractures
Her discharge summary also contains worrying blood test results that still need investigating
“Years ago, they would’ve sorted it in hospital,” says Greg
“Now it’s, ‘GP, deal with this.’ You’re picking up the pieces, making sure they’re safe at home and chasing all the tests.”
This consultation takes around 20 minutes, double the recommended 10, followed by more paperwork
The next patient is a suicidal young person
“We have loads and loads of mental health problems, especially in younger people,” he says. “There are no real support services. Mental health services are so poor that they just come to us.”
In the next hour he could see patients worried about infertility, cancer and suicide
“Every patient is complicated,” he says. “The hospital keeps pushing work into general practice because they can’t cope, but we can’t say no.”
He recalls referring a man with chest pains to hospital after deciding something did not feel right. The man later died of a heart attack
The case still haunts him, and the constant pressure of making those calls takes its toll
“Every 10 minutes you’re making really big decisions. By the end of the day my decision-making capacity is completely gone. I can’t even think about what to eat for dinner sometimes so I just end up grabbing McDonald’s.”
‘You will burn out’
A legacy of how general practice was established means GPs work differently from most NHS staff
Unlike other NHS workers, most GP practices operate as independent businesses contracted to provide NHS services
The BMA breaks down GPs’ work into “sessions”, each of which lasts four hours and 10 minutes. It defines full-time as nine such sessions a week, or 37.5 hours
Yet official figures show that just 7,314 of England’s 39,044 fully qualified GPs work that pattern
For many, reducing hours is not a lifestyle choice but a survival strategy
Greg, who is in his 30s, wanted to work as much as possible after training and working in A&E, but says colleagues actively warned him against it
“I want to work full-time, but everyone said if you do more than six sessions, you will burn out and leave within a few years.”
On paper, Greg earns around £77,000 for just under 25 hours of contracted work a week
Critics argue that fewer sessions affect continuity of care and access to appointments. But Greg says he routinely works 11-hour or 12-hour days as rising demand, an ageing population and increasingly complex patients have transformed the job
According to the BMA, every full-time GP is responsible for around 2,000 patients, rising to almost 2,600 in London
This rise is partly fuelled by soaring immigration piling pressure on an already stretched workforce
Professor Victoria Tzortziou Brown, chairman of the Royal College of GPs, says the rise in part-time working reflects the changing reality of modern general practice
“This is not about working less; it is about working in a way that is safe and sustainable.”
Official definitions also tell only part of the story
Research published in the British Journal of General Practice found that fewer than 10pc of GPs worked the BMA’s nine-session definition of full-time in 2021
Using the NHS Careers definition of an eight-session week, the figure rises to 29.4pc, while almost two thirds worked at least the Government’s standard 35-hour week
Paperwork piles up
The shift towards part-time working is particularly pronounced among younger doctors
Just 11pc of fully qualified GPs aged under 40 now work full-time, compared with 19pc in 2019
Many are combining clinical work with teaching, writing or even private or locum work in the same surgeries
Martin Brunet, 58, has watched that change unfold over 25 years at the same surgery in Godalming, Surrey
He still remembers when he could play squash during his lunch break. Now, he jokes, he brings his food in simply to ensure he has time to eat
Like many GPs, Brunet has reduced his clinical sessions
He believes the appeal of fewer NHS sessions for younger doctors is not simply working less, it is escaping the growing administrative burden that comes with being a GP partner or salaried doctor
Locum and private work can offer longer consultations and far less paperwork
But Brunet argues the change cannot be understood without looking at how much general practice itself has changed. When he started, consultations were often just five minutes
“If you look at the notes GPs wrote 35 years ago, they would just write ‘whooping cough’ and that would be the entire record. The doctor was largely deciding what was wrong and telling the patient what to do.”
There were fewer regulations, less paperwork and fewer treatments to manage
“You could see 40 or 50 patients a day, but it was a very different world,” he says
Today, consultations are longer because patients are older, conditions are more complex and medicine has expanded into areas that barely existed in everyday general practice when Brunet began.“We were never talking to people about ADHD or autism. There’s just so much more that is complicated now.”
The Royal College of Psychiatrists estimates that around 25pc of GP appointments involve mental health conditions
The result is a contradiction at the heart of modern general practice: consultations have doubled in length, but the demands packed into each one have multiplied
“Most consultations have gone to 15 minutes now. Realistically, 20 to 30 minutes per patient would be amazing, but then you can’t get through everyone who needs to be seen that day.”
And the work does not end when patients leave
“My day will often be an eight-to-eight day. I’ll clear the urgent admin, but I’ll still have letters to write and things to finish.”
Even on days off, Brunet often logs back in from home to spend another four hours clearing the backlog
Would-be GPs left jobless
The pressures GPs face explain why many are reducing their hours
But they do not explain another puzzle at the heart of general practice: while patients struggle to see a doctor, some qualified GPs are struggling to find work
Becks Fisher, of the Nuffield Trust, says part of the explanation lies in the rapid expansion of non-GP roles through the Additional Roles Reimbursement Scheme (ARRS), introduced in 2019 to bring more staff into general practice
“In the past five years, government have funded a massive expansion of non-GP staff in general practice: roles like physios, paramedics and pharmacists
“They weren’t really meant to replace GPs, but they are part of the problem of GP unemployment,” she says
Until 2024, practices could use ARRS funding for these roles but not for salaried GPs. At the same time, the number of newly qualified doctors was rising
“We’d finally succeeded in getting healthier training pipelines for GPs, so more were qualifying each year with over 4,000 newly qualified GPs in 2024 compared with more like 2,700 per year in 2015.”
Advertisement
Fisher says this created a mismatch: more GPs entering the workforce, but limited funding for practices to employ them
“You had this perfect storm of lots of GPs looking for jobs, and GP partners essentially saying, ‘Why should we pay from our own money to employ GPs, when we can employ other staff at no cost to ourselves?’”
Changes allowing ARRS funding to be used for GPs have helped, she says, but the imbalance remains
“Whereas a few years ago there were far more GP jobs than there were GPs to fill them, we still have unemployed and underemployed GPs now.”
The expansion of other roles in surgeries has also changed general practice
While staff such as physios or pharmacists can take on some simpler appointments, GPs are increasingly left managing the most complex cases
Stuart Hoddinott, from the Institute for Government, says: “It does take appointments off GPs’ plates, but those are often the lower complexity appointments, and it leaves GPs with the more complex ones.”
The result is that doctors may see fewer routine cases but face a heavier clinical burden
“Maybe before, 20pc of those would have been renewing a prescription or just chatting to Mrs Jones about doing some exercises after a hip replacement, and now all of them are quite complex cases and you’re having to make quite difficult decisions.”
Digital drive
Rising demand and pressure on GP capacity have inevitably led to a shift away from in-person appointments
However, this shift has also fuelled patient frustration, ranging from elderly people struggling with online systems to fears that important decisions are being reduced to digital tick boxes and remote assessments
Patients are increasingly triaged before seeing a doctor, with reception teams, online forms and other professionals often acting as the first point of contact
Around two thirds of GP appointments are now face-to-face, with the remaining third taking place over the phone or online. That is compared to four in five appointments being face to face before the pandemic
Steve Mowles, a GP partner who manages a busy practice in Lambeth, south London, already has 38 patients to see when we talk on Monday
He adds that a decision by the former health secretary Wes Streeting to lift a cap on the number of electronic consultations has placed additional strain on practices
“You could potentially have 100 extra electronic consultations coming in on any given day, and you just have to deal with it. At what point does the workload become unsafe?”
Greg says online systems have also created a generational divide. Older patients can struggle with digital forms, while younger ones, used to instant online access, fill in several at a time, expecting healthcare to work the same way
The internet has also changed demand. A quick Google search can turn a headache into a deadly disease within minutes, while patients increasingly arrive armed with information and their own diagnosis
Sick note culture
And then there are sick notes – or “fit notes” as they’re now known
Greg says he has developed a sixth sense for when a consultation is heading towards a request
Within minutes, he can often tell when a patient who has arrived with a long list of vague symptoms is not just looking for a diagnosis, but hoping to leave with a note signing them off work
“They’ll have all these problems, all these symptoms, and then you basically just often can’t really work out what they’re after. Nothing really feels like a medical problem at the end.”
Eventually, Greg says the reason for the appointment becomes clear. “Then you’re like, ‘OK, you’re after a fit note!’”
He says he has refused notes in the past and cut some short, but it puts him in an uncomfortable position
“At the end of 14 patients in the morning and 14 patients in the afternoon, the last thing you want to do is have a 15th patient and argue about whether or not they’re fit to work.”
He says the problem is that GPs are being asked to make decisions for which they are not best placed
“I can give them a fit note, but I shouldn’t be the one who tells them whether or not they can work, because I don’t know what demands their workplace puts on them.”
It’s little wonder, then, that the vast majority of workers who ask for a fit note are signed off work. Official figures show that more than 11 million fit notes were issued last year, with 93pc declaring employees unfit to work
Greg believes doctors should diagnose and treat conditions,while occupational health specialists or others should decide whether someone is fit to return to a particular job
The Government has started piloting schemes that replace fit notes with support to help people stay in their jobs
Mowles also believes a separate service could provide a more objective assessment and, in some cases, help people return sooner
“As a family doctor, we’re advocates for our patients, we’re there to care for them. If we’re getting into potentially challenging conversations about whether you should be going back [to work], that changes that relationship.”
He argues that an independent assessment could help remove some of that tension
“In reality, I think there probably are quite a lot of people who need help back to work earlier if there was a really objective assessment about it.”
Temptation to work abroad
The figures appear to suggest a uniquely British problem: doctors in the UK are less likely to work full-time than some of their overseas counterparts
Around 17pc of British doctors work full-time, compared with 28pc of doctors from South Asian backgrounds
But Greg argues the question is not simply whether doctors want to work more, it is whether the system makes that possible
He says he has considered working abroad, where the combination of pay and working conditions can be far more attractive
Australia, in particular, has become a major draw for UK-trained doctors, who are often able to earn significantly more while working fewer hours
Greg’s £77,000 salary currently includes an £11,000 top-up – the equivalent of an extra GP “session” – to reflect his longer working hours. It was offered to him when he qualified
However, this extra financial perk runs out after a year. Greg says he will consider his next move once the bonus is taken away
GPs in Australia can earn double what they command in Britain, although he says general practitioners are less welcome than A&E doctors
Greg adds that his family and a close circle of friends are the only things keeping him here
“My wife and I have thought about it a little bit. It’s difficult because our family are all here, and we want to be in the UK long term. But for work, it would be a no-brainer if our family was in Australia.”
He says his wife, who is also a doctor, regularly receives messages from recruiters offering overseas positions
“She gets loads of emails from recruiters asking, ‘Do you fancy ridiculous amounts of money for four days a week and a great lifestyle?’ And we’re like, ‘Stop sending us emails!’”
The pull of overseas work comes alongside concerns about the financial incentives within the NHS itself. Mowles says tax thresholds can discourage some doctors from taking on additional sessions
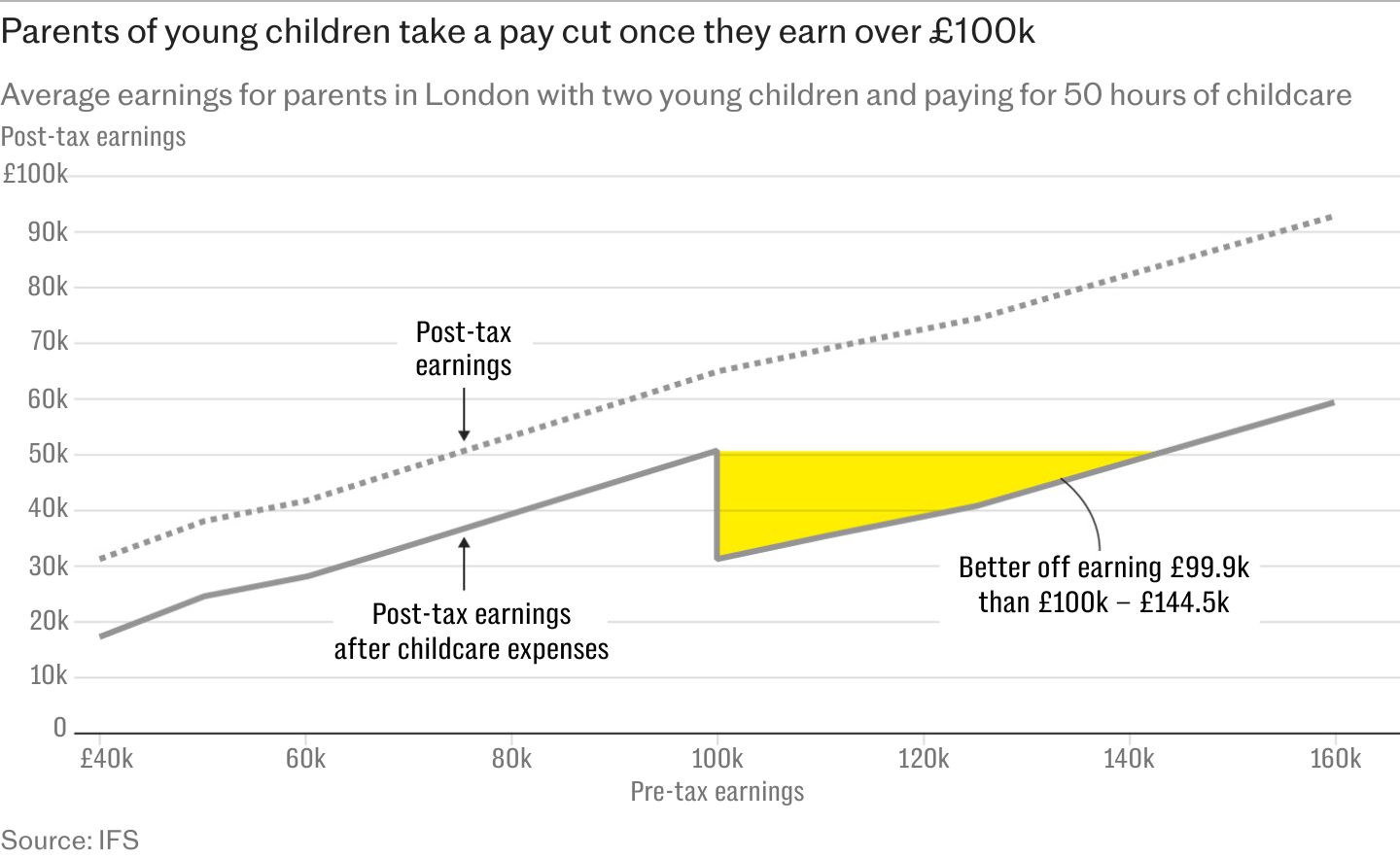
Some doctors approaching the £100,000 income threshold can face losing childcare support and personal tax allowances in a stroke of a pen, meaning extra work may not translate into a meaningful increase in take-home pay
“There are early-career GPs who could work more, but they hit that £100,000 level and actually they lose childcare support and personal tax allowances. It is a major disincentive.“There needs to be a way to incentivise younger GPs who hit that level to be able to work more, and also retain GPs towards the end of their career.”
The personal cost
For Alia Fahmy, the breaking point came when she walked into work and saw more than 100 patients on the on-call list, with a 17-hour day ahead if everything went to plan
After years as an NHS GP in Leamington Spa, Warwickshire, she felt the system had become unsustainable
The pressure was not only clinical: long days inevitably meant missing her daughters growing up
In August 2020, during the pandemic, she left NHS general practice for private medicine, where she now works as a medical director
“It was missing out on pretty much everything [that made me leave]. School plays, things with my kids, and realising that I was essentially an absent mother. That’s not what I wanted.”

She says the shift towards telephone triage during lockdown changed the nature of the job. If she decided she needed to see a patient after a telephone call, she would not be allocated any extra time
“You were almost punished for actually physically wanting to see and examine your patients, which is a bit counterintuitive when you go into practice medicine and you’re learning all your clinical skills based on examination.”
A typical NHS day could run from 7.30am to 7.30pm, with appointments, home visits, prescriptions, letters and test results creating a constant backlog
Today, Fahmy works in a home-visiting service where doctors look after a much smaller number of households rather than thousands of registered patients
“We have a limit on how many patients our doctors can look after, and that’s 200 households.”
She says the model allows her to spend longer with patients and provide continuity that has become harder in NHS general practice
For Fahmy, the biggest difference is going back to a family doctor model that only older generations remember
“If you want doctors to do more hours for the NHS, you need to make sure those hours are less chaotic. That means reducing the number of patients they’re expected to see. And that means having more GPs,” she says
The pressure is also being compounded by wider NHS problems, particularly record hospital waiting lists. Since January 2020, the NHS waiting list has grown from 4.4 million to 7.3 million cases, with around a third of patients now waiting longer than the 18-week target, compared with around 16pc before the pandemic
Brunet says the knock-on effect lands back in general practice
“One thing that is definitely impacting general practice is waiting lists, because if someone has to wait a year for their hip replacement, what do we do in the meantime? Try not to get them hooked on strong painkillers when they’re really upset and in pain.”
For Fahmy, it is little surprise that more doctors and patientsare looking to go private
Private admissions reached a record high in 2025, with around 953,000 people paying for treatment, according to the Private Healthcare Information Network
The strain is also showing among NHS staff themselves. Anxiety, stress, depression and other psychiatric illnesses were the leading cause of sickness absence across the health service in the year to March 2026, accounting for almost three in 10 absences
On Monday morning, Greg will once again sit down in front of a screen full of names, knowing every 10 minutes could bring another life-changing decision
The question is not whether Britain has enough people willing to become GPs. It is whether the NHS can build a system that persuades them to stay